Hormones
Can I have too much Estrogen?

Estrogen dominance describes a state where estrogen’s effects are relatively high compared with progesterone, and this imbalance can amplify PMS, PMDD‑like symptoms, and estrogen‑driven conditions like endometriosis.
What exactly is “estrogen dominance”?
Clinically, most endocrinology texts do not list “estrogen dominance” as a formal diagnosis, but many clinicians and researchers use it as a shorthand for a high estrogen‑to‑progesterone ratio and the symptoms that come with it. The U.S. Veterans Affairs Whole Health Library defines it as a state of increased estrogen relative to progesterone, driven by overproduction, impaired breakdown, or changes in estrogen metabolism and excretion.
Biologically, estrogen acts through estrogen receptors in target tissues across the body—including the uterus, breast, brain, bone, and cardiovascular system—to regulate cell growth, mood, metabolism, and more. When estrogen’s actions are not adequately balanced by progesterone, tissue growth and inflammatory signaling can become amplified, which is relevant in heavy periods, breast symptoms, and conditions like endometriosis.
What hormones are actually involved here?
The key players are estradiol (the main reproductive estrogen), progesterone, and the receptors and enzymes that metabolize these hormones. Estradiol stimulates growth of the uterine lining and affects neurotransmitters like serotonin and GABA, while progesterone normally counterbalances this by stabilizing the lining and exerting calming effects on the brain.
“Estrogen dominance” often means one of three things: estrogen is too high, progesterone is too low, or both are “normal” but out of balance relative to each other. This ratio can shift in anovulatory cycles (no ovulation, so very little progesterone), perimenopause, polycystic ovary syndrome (PCOS), thyroid dysfunction, and in some people exposed to external estrogen‑like compounds.
What are the most common symptoms of estrogen dominance?
Because estrogen receptors are widespread, symptoms range from strictly menstrual to whole‑body.
Typical estrogen‑dominant symptom cluster:
Heavy or prolonged periods, clotting, irregular cycles.
Worsened PMS: bloating, breast tenderness, irritability, mood swings.
Full or tender breasts, dense breast tissue.
Pelvic pain, endometriosis, fibroids, or endometrial hyperplasia in some.
Fluid retention, weight gain or difficulty losing weight, particularly around hips and thighs.
Sleep disturbance, fatigue, brain fog, low libido, and headaches.
Medical organizations also note that estrogen‑related imbalances are implicated in uterine fibroids, endometriosis, and certain estrogen‑sensitive cancers, which is one reason clinicians pay attention to this pattern even if they don’t code “estrogen dominance” as a diagnosis.
How is estrogen dominance different from “normal” hormone fluctuations?
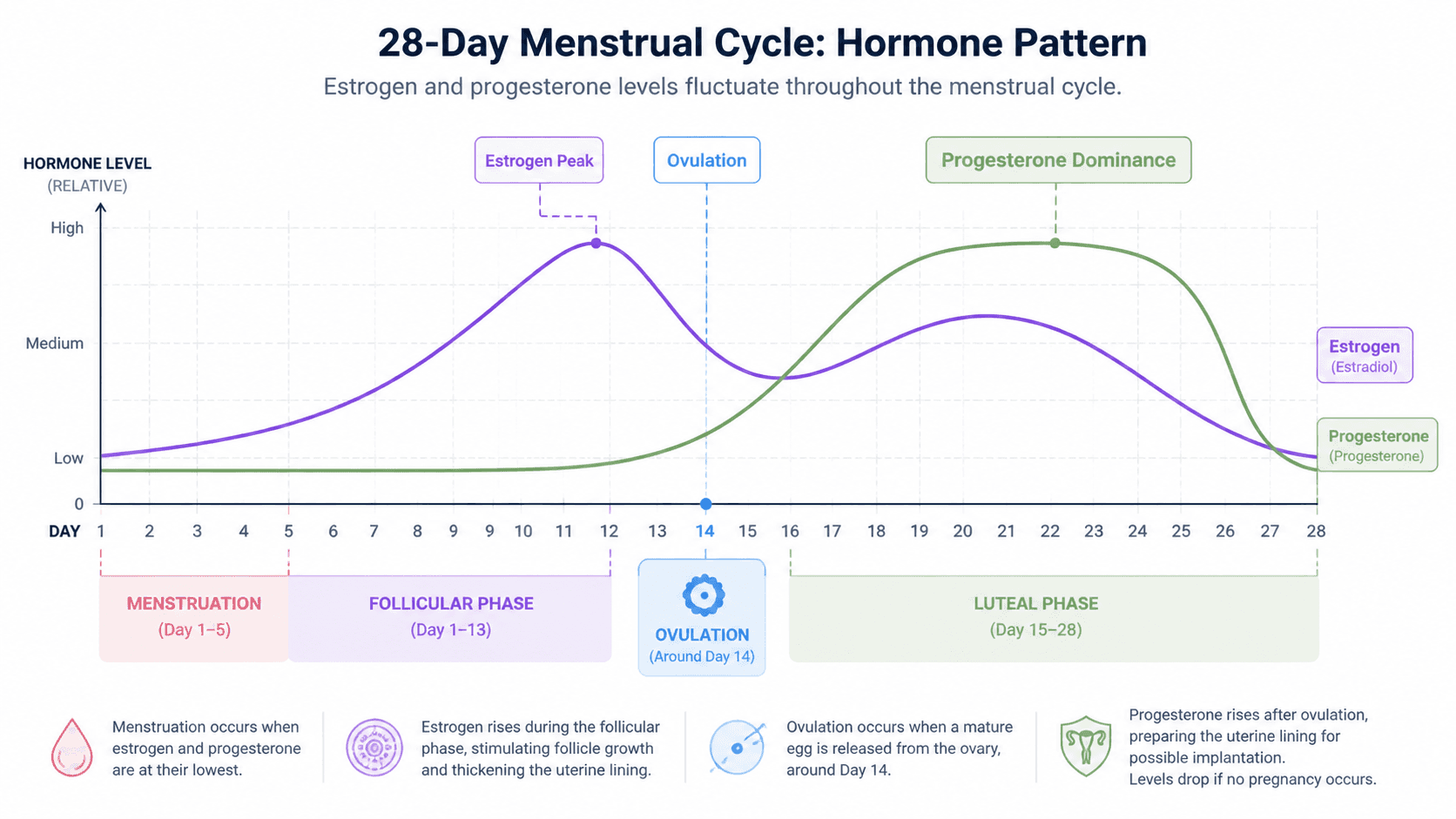
Throughout a healthy cycle, estrogen rises in the first half, peaks around ovulation, dips, then rises again, and progesterone dominates the second half (luteal phase). This ebb and flow is normal; symptoms are usually mild and manageable.
Estrogen dominance describes when that natural choreography becomes skewed—estrogen peaks are higher, progesterone is too low or mistimed, or tissues are unusually sensitive to estrogen’s effects. For example, chronic anovulation (common in PCOS and perimenopause) leads to ongoing estrogen exposure without the balancing progesterone surge, which can drive heavy bleeding and premenstrual symptoms.
What causes estrogen dominance in the first place?
Experts describe several overlapping drivers rather than a single cause.
Anovulatory or irregular cycles: PCOS, perimenopause, and some hypothalamic conditions reduce or eliminate ovulation, so progesterone stays low while estrogen still circulates.
Impaired estrogen metabolism: The VA Whole Health Library notes that changes in how the liver and other tissues metabolize estrogen, shifting away from “safer” metabolites (like 2‑hydroxyestrone) toward more proliferative forms, can contribute to estrogen‑dominant states.
Endocrine and thyroid disorders: Thyroid dysfunction can slow estrogen clearance, contributing to higher effective levels over time.
Body fat and insulin resistance: Adipose tissue produces estrogen via aromatase, and insulin resistance (as in some PCOS cases) can alter estrogen and androgen metabolism.
Medications and exogenous estrogens: Some hormone therapies and environmental endocrine disruptors can increase total estrogenic activity.
A 2018 review in Gynecologie Obstetrique Fertilite & Senologie described how excess estrogen signaling and receptor overexpression can promote tissue growth and increase risk of certain hormone‑sensitive diseases, underscoring why balance matters.
How can estrogen dominance show up as PMS?
Premenstrual syndrome (PMS) involves cyclic emotional and physical symptoms that impair quality of life in the luteal phase. While PMS is multifactorial, estrogen‑progesterone imbalance can intensify these symptoms: high estrogen with relatively low progesterone has been linked to more severe mood swings, bloating, breast tenderness, and headaches.
The VA Whole Health Library notes that estrogen‑dominant patterns are associated with more intense PMS, and conditions like fibroids and endometriosis, suggesting that estrogen’s proliferative and inflammatory actions may exacerbate premenstrual symptoms. Some functional and integrative clinicians also observe that stabilizing the estrogen‑progesterone ratio can reduce PMS severity, though high‑quality randomized trials are still emerging.
Does estrogen dominance cause PMDD?
Current evidence suggests that most people with PMDD have normal hormone levels, but their brains are unusually sensitive to the normal rises and falls of estrogen and progesterone. The International Association for Premenstrual Disorders and peer‑reviewed reviews emphasize that hormonal “numbers” are typically in range, and what changes is the central nervous system response.
That means estrogen dominance is not considered a primary cause of PMDD by major medical bodies, even though some people with PMDD‑like symptoms may also show estrogen‑dominant patterns. Instead, research points to altered sensitivity of GABA and serotonin systems to progesterone’s metabolites and estrogen’s modulation of those pathways, which can amplify mood symptoms in susceptible individuals.
How can estrogen dominance be evaluated by a healthcare professional?
There is no single universally accepted “estrogen dominance test,” and organizations like the VA note that formal lab testing is often unnecessary for many women. Instead, clinicians usually combine:
Symptom history (bleeding pattern, PMS severity, pelvic pain, breast changes).
Cycle tracking (whether ovulation is occurring, luteal phase length).
Targeted labs when indicated—such as estradiol, progesterone, thyroid function, prolactin, and sometimes androgen and insulin markers.
You can find ration on your own using this link as well.
When conditions like endometriosis, fibroids, or endometrial hyperplasia are suspected, imaging or surgical evaluation may be recommended according to gynecological guidelines, since these are structural consequences of long‑term estrogen‑dominant environments. We recommend tracking your cycle and symptoms using HealCycle app.
What lifestyle factors can help support healthier estrogen balance?
Official resources emphasize general lifestyle pillars that also improve estrogen metabolism and reduce risk of hormone‑sensitive conditions.
Nutrition to support liver and gut: Diets rich in fiber, vegetables, and cruciferous plants (like broccoli and cabbage) can support estrogen metabolism
Physical activity and weight management: Maintaining a healthy body weight helps reduce aromatase activity in adipose tissue and may lower total estrogen burden.
Limiting alcohol and smoking: These behaviors can impair liver processing of hormones and have been linked to altered estrogen metabolism and increased cancer risk.
Managing endocrine disruptor exposure: Professional bodies highlight concerns about certain environmental chemicals with estrogen‑like activity, reinforcing the importance of reducing unnecessary exposures where possible.
These strategies are not cures, but they are broadly recommended components of whole‑person care for estrogen‑sensitive conditions.
How do symptoms of estrogen dominance, PMS, PMDD, and endometriosis compare?
Feature / Symptom | Estrogen‑dominant pattern (high E: low P) | PMS | PMDD | Endometriosis |
|---|---|---|---|---|
Core driver | High estrogen relative to progesterone. | Normal fluctuations with mild sensitivity. | Normal levels, extreme brain sensitivity to hormones. | Estrogen‑dependent, progesterone‑resistant lesions. |
Bleeding pattern | Heavy, prolonged, sometimes irregular. | Usually normal to mildly heavier. | Usually normal pattern. | Heavy or painful periods, spotting, sometimes normal. |
Pain | Cramps, breast tenderness, headaches. | Cramps, breast tenderness. | Marked mood symptoms; pain can coexist. | Chronic pelvic pain, deep dyspareunia, bowel/bladder pain. |
Mood symptoms | Irritability, anxiety, mood swings.va+1 | Mild to moderate mood changes. | Severe depression, rage, anxiety, suicidality. | Pain‑related mood changes; not primary driver. |
Timing in cycle | Often throughout, worse premenstrually. | Luteal phase, resolve with menses. | Luteal phase, resolve quickly after menses starts. | Often worsens around menstruation and ovulation. |
Which symptoms suggest I should see a doctor urgently?
While mild PMS and cyclical breast tenderness can be monitored, certain symptoms warrant prompt medical evaluation.
Very heavy bleeding (soaking through a pad or tampon every hour for several hours, or passing large clots).
Bleeding between periods or after sex.
Severe pelvic pain, especially if sudden or worsening over time.
Breast lumps, nipple discharge, or skin changes.
Symptoms of anemia (shortness of breath, dizziness, extreme fatigue) from heavy periods.
These signs may point to structural conditions like fibroids, endometriosis, or, rarely, malignancy, and should be assessed using established gynecologic and oncology guidelines.
References
Latest
From the Blog
Discover fresh insights, practical tips, and empowering stories to help you learn and grow in your PMDD healing journey. We're always here to remind you that you're not alone



